A standard specialized surgical platform weighs 1,800 pounds, costs upwards of $2 million, and locks a healthcare provider into a single-purpose capital asset depreciation cycle. In July 2026, researchers at the University of California San Diego bypassed this entire infrastructure paradigm. By mounting mechanical adapters onto a pair of mass-market Chinese humanoid robots—the Unitree G1—and routing human-driven telemetry through custom translation software, the team executed a laparoscopic cholecystectomy on a live porcine subject.
The immediate temptation is to frame this as an achievement in artificial intelligence or autonomous medicine. It is neither. Every incision, retraction, and clip application was teleoperated by a human surgeon in real time. The true value of the UCSD experiment lies in its structural subversion of medical hardware economics: the successful decoupling of specialized surgical kinematics from specialized surgical machinery.
The Capital Expenditure Arbitrage
To understand the strategic shift demonstrated at UCSD, one must analyze the physical and financial constraints of current robotic-assisted surgery (RAS). Market-leading platforms utilize a dedicated architecture. The mechanical arms, the control console, and the data bus are structurally integrated, requiring dedicated, retrofitted operating suites. This creates a high capital expenditure barrier that restricts advanced minimally invasive surgery to high-volume urban medical centers.
The Unitree G1 platform operates on a different economic model. A base general-purpose humanoid unit retails for approximately $13,500. Even when configured with three-fingered dexterous hands optimized for tool manipulation, the hardware cost scales to roughly $67,000.
This creates a distinct hardware-software cost function:
- Dedicated RAS Platform: High fixed asset cost + low adaptation flexibility.
- General-Purpose Humanoid Platform: Low fixed asset cost + high software adaptation investment.
By utilizing a 60-pound, 5-foot-tall mobile form factor, the system shifts the deployment constraint from specialized physical infrastructure to simple digital connectivity. The physical footprint fits into spaces designed for human staff, which eliminates the structural retrofitting costs that stymie the deployment of traditional surgical robots in rural clinics, forward military positions, or field hospitals.
Kinematic Translation and Structural Bottlenecks
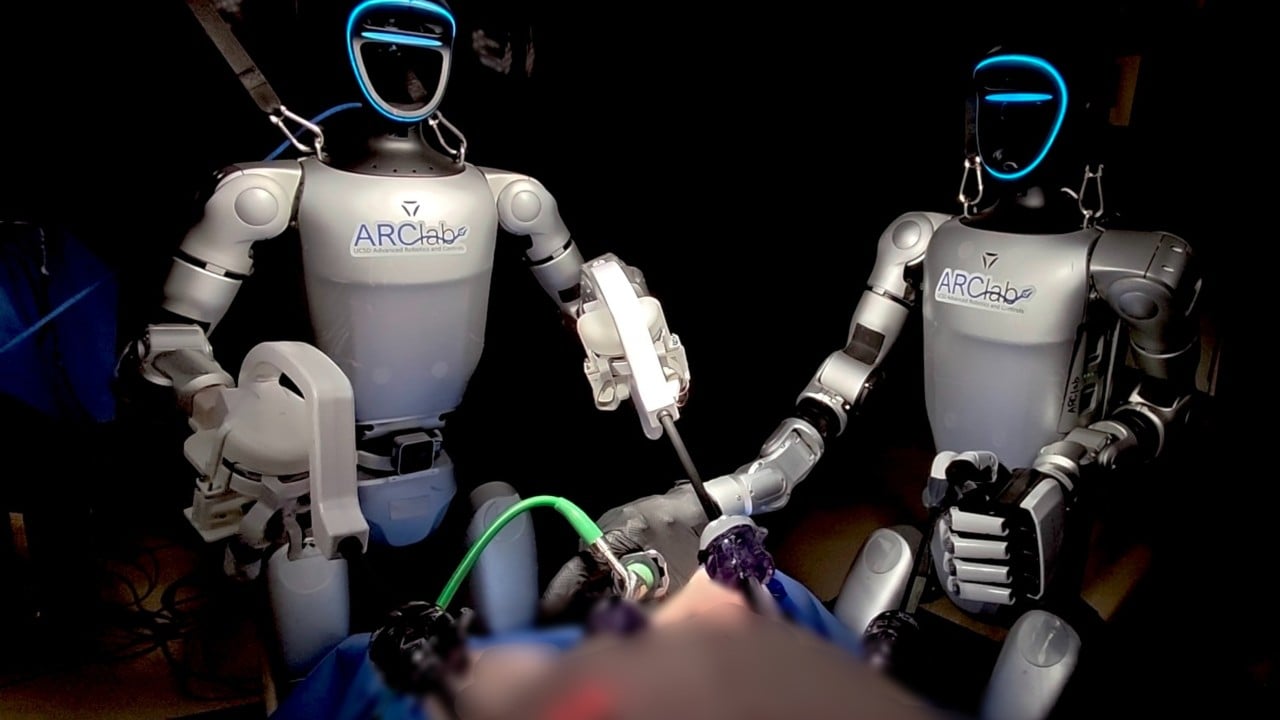
The UCSD team executed two distinct surgical configurations: a human-robot hybrid team (one humanoid acting as primary operator with a human assistant) and a dual-robot team (two humanoids operating in tandem, one handling the endoscope and tissue retraction while the other performed dissection).
The core engineering hurdle is not the generation of autonomous intent, but the mapping of human kinematic commands onto an off-the-shelf robotic chassis that was never engineered for sub-millimeter precision.
[Surgeon Input Console] ──> [Translation Software] ──> [Mechanical Adapter] ──> [Standard Surgical Tool]
This translation pipeline introduces three structural bottlenecks that currently prevent clinical deployment on human patients.
Spatial Span and Mechanical Leverage
The Unitree G1 features an arm span of approximately 450 millimeters, roughly a quarter of the reach of a human adult. This condensed kinematic envelope limits the working radius of the robot. During the procedures, this forced tighter positioning of the units relative to the operating table, compressing the physical workspace and increasing the risk of external mechanical collisions between the dual units or human assistants.
Drift and the Recalibration Penalty
Unlike specialized surgical systems that use high-resolution closed-loop optical encoders to track arm positioning perfectly over hours of operation, general-purpose humanoids experience micro-drifts in joint calibration under sustained loads. The UCSD researchers had to pause the procedures multiple times to run calibration routines.
This introduces a severe time penalty. While a mature, specialized platform allows a modern laparoscopic gallbladder removal to be completed in roughly 30 minutes, the humanoid-driven procedures ran significantly longer. This duration inflation directly increases the patient's exposure to anesthesia, compounding clinical risk.
Latency Profiles
Safe surgical teleoperation requires an end-to-end telemetry delay of under 150 milliseconds to ensure the surgeon’s visual feedback matches their haptic or physical inputs. The off-the-shelf communication stack on general-purpose humanoids introduces hundreds of milliseconds of latency. In practice drills, both expert surgeons and residents consistently registered slower completion times on the humanoid rig than on standard laparoscopic or specialized robotic setups. The delay creates an operational drag, forcing the operator to adopt a slower "move-and-wait" strategy to avoid over-correcting tissue tension or accidental tissue shearing.
The Structural Path to Clinical Feasibility
The hypothesis that general-purpose hardware can eventually replace single-purpose surgical systems relies on a historic precedent. The first specialized robotic laparoscopic surgeries performed decades ago took upwards of six hours before engineering refinements compressed that window to the current 30-minute standard.
For general-purpose humanoids to follow a similar optimization curve, the development roadmap must prioritize three specific technical milestones:
- Direct Tool Integration: Eliminating the mechanical hand-to-tool interface entirely by swapping out the multi-purpose hand for a direct-drive surgical instrument quick-connect bayonet.
- Hard Real-Time Operating Systems (RTOS): Stripping down the robot's onboard communication protocols to prioritize low-latency motor-command pipelines over general-purpose background processes.
- Local Closed-Loop Compensators: Implementing micro-optical tracking at the tool tip to automatically correct for joint drift without requiring the surgeon to halt the operation for manual system recalibration.
The long-term objective of this research track is not to achieve fully autonomous AI surgeons, but to democratize the physical delivery of specialized surgical skill. The true value metric is access expansion. If a $67,000 general-purpose robot can perform at 90% of the kinematic efficacy of a $2,000,000 single-purpose platform, the geographic distribution of advanced surgical care changes entirely. Hospital networks will no longer look at surgical robots as centralized capital investments, but as distributed mobile appliances deployed to any room, clinic, or field location reachable by a broadband data link.



